
If you’re considering breast augmentation or implant revision, one important decision you and your surgeon will need to make together is whether to place your new breast implants over or under your chest muscle. This placement matters for a number of reasons, and to help guide you in making this decision, board-certified plastic surgeon Dr. Movassaghi explains the differences between over and under the muscle breast implant placement in this post.
How do breast implant placement options compare?
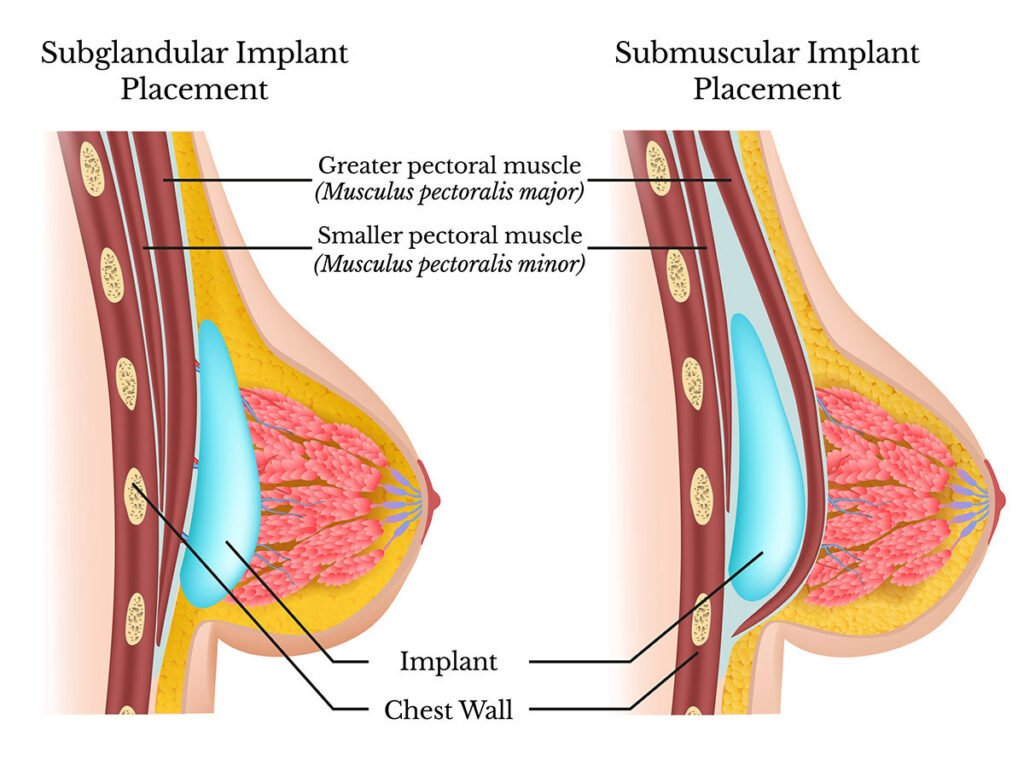
Breast implant placement is critical to providing a patient with the best aesthetic results, as well as to prevent issues, such as capsular contracture and implant rippling, from occurring. During breast augmentation surgery, breast implants are either placed underneath a patient’s breast tissue but over their chest muscles, or underneath their breast tissue and partially under their pectoralis major chest muscle. Placement in both locations can produce satisfactory results; however, there are pros and cons to each option, therefore your surgeon will assess your unique body type to determine which implant position is right for you.
Over the muscle placement
Subglandular, or “over the muscle,” implant placement is when a breast implant is placed on top of a patient’s muscles but beneath their skin, fat, and glandular tissue.
Pros of subglandular placement:
- Recovery is usually easier than recovery from submuscular placement.
- Chest muscles remain intact, therefore there is no loss of function or weakness.
- Final results are usually achieved within a few weeks.
- Able to accommodate larger implants.
Cons of subglandular placement:
- Although some studies show that the use of smooth implants in subglandular placement very frequently results in capsular contracture (roughly 10.6% of patients), this is being debated as more data is emerging. My personal capsular contracture rate for subglandular placement is only 1-2%.
- Implant rippling—when “wrinkling” is visible on the outer perimeter of an implant—may occur during subglandular placement because it is easier to see the upper “edges” of the implants when they are placed over the muscle. Implant rippling is most commonly seen in thinner women with smaller breasts, as they have less breast tissue to hide their implants. Implant rippling can often be avoided by working with a board-certified plastic surgeon who understands how to properly choose and place implants. In fact, in patients who are thin and choose to have subglandular augmentation, I can help them with the upper pole fullness by injecting their own fat borrowed from another part of the body, like the belly or hips.
- Subglandular implants interfere more with mammogram readings, although there are other modalities, such as ultrasounds, that can improve mammogram results.
Under the muscle placement
The term submuscular, or “under the muscle”, implant placement is somewhat misleading: while the breast implant is placed underneath a patient’s skin, fat, glands, and pectoralis major muscle (the outermost chest muscle), most surgeons actually place the implant on top of the inner pectoralis minor and serratus muscles so that the pectoralis major muscle covers the top and side of the implant. This leaves the bottom and outer edge of the implant covered only by the patient’s natural breast tissue.
Pros of submuscular placement:
- Provides more tissue coverage over the implant in the upper pole.
- Creates a smoother transition from the chest wall to the implant.
- Achieves the most natural-looking result.
- Submuscular implants interfere less with mammography.
Cons of submuscular placement:
- Your surgeon will have to cut and detach your pectoralis major muscle.
- Implants may become distorted when the chest muscle contracts.
- Higher chance of the implant migrating upwards and towards the armpit.
- Higher chance of secondary deformities, such as “double-bubble” deformity, along the lower pole of the breast.
- Slightly longer and more uncomfortable surgery and recovery period.
- Diminished strength in the chest muscles after surgery.
Breast revision: the other reason to consider implant placement
If you’ve already had a breast augmentation, you may be researching implant placement options because you’re interested in revising your breast implants. Breast revision surgery is often performed to exchange breast implants, but it can also be performed to correct common issues that occur over time, such as loose breast skin, as well as other issues that can develop, like implant migration, implant rippling, and/or capsular contracture (when the scar capsule around the implant constricts). During breast revision surgery, you and your surgeon may decide to change the placement of your implants to accommodate a new implant size or to correct any of these issues.
How do I decide where to place my breast implants?
Now that you are familiar with the two main breast implant placement options, how do you choose which one is best for you? Here are a few factors that will help inform your decision:
How much breast tissue and chest muscle you have
Just as thinner women with less breast tissue may be better candidates for submuscular placement, women who have very large and/or strong chest muscles are better suited for over the muscle implant positioning. This is because women with larger chest muscles will have a greater chance of distorting their implants as their chest muscles move and contract. Women with more breast tissue are also better candidates for subglandular implant placement because their natural tissue can better hide their implants.
To find out if you may have adequate tissue for over the muscle implants, Dr. Movassaghi recommends doing a basic pinch test. Here’s how it works: With your thumb and pointer finger, pinch the skin right above your upper pole (the very top of your breast); if the amount of skin you can grab is 2cm or more, you’re likely a good candidate for both options. If you have less, you’ll likely need to consider under the muscle placement or adding fat to the upper pole to increase skin thickness in that area.
In addition, women who are very athletic and active may choose subglandular implant placement in order to eliminate any chances of muscle weakness. Sometimes, a smaller implant with less projection can be a good compromise for these individuals.
The size of your implants
When choosing the size of the implant, it is more important to think about the shape of the breast you want instead of the amount of CC’s in the implant. My approach is to shape your breast rather than to volumize it. There are some general guidelines that are important when considering implant placement because the larger your implants are, the more likely any rippling is to be visible through your breast tissue. This is why women with larger breasts and more abundant breast tissue are better candidates for larger implants, while women with smaller breasts may have a more difficult time concealing larger implants. Generally, if you have minimal breast tissue and want larger implants, under the muscle placement will provide the best results as your pectoralis major muscles will help hide any possible rippling in your implants. It’s important to understand that as the size of your implants increase, so does your rate of short-term and long-term complications, and correspondingly, your chances of seeking an implant revision.
Saline vs. silicone breast implants
In general, silicone implants are less prone to rippling and visibility. There are also more options for silicone implants, both in size and shape and in gel materials. That said, there have been recent improvements to saline implants which make them ripple less and feel more natural than older versions. The options for saline implants are, however, more limited.
Your individual goals and desires
There are many factors to consider when choosing your implant size, shape, and location. Your anatomy, the ultimate shape and size of the breast you desire, and your lifestyle all play an important role in your decision. Remember, there is no “one-size-fits-all.” Together, we will decide on the right implant and implant location to achieve your goals during your consultation.
What is the most popular implant placement option?
There is no “Holy Grail” for implant type, size, shape, or location. What is right for one individual may not be right for another. In fact, Dr. Movassaghi just recently published a book titled, “Shaping the Breast: A Comprehensive Approach in Augmentation, Revision, and Reconstruction,” to address this exact issue, among others.
Ready to discuss your implant placement options in Eugene? Consult Dr. Movassaghi
If you’re still unsure which implant placement option is right for you, don’t worry. During your consultation, board-certified plastic surgeon Dr. Kiya Movassaghi will measure your breast tissue thickness and help you understand your breast implant placement options in detail. Dr. Movassaghi has over 19 years of experience lecturing and performing breast augmentation and breast implant revision surgeries and would love to help you achieve your ideal augmentation results. Contact our Eugene office online or call (541) 686-8700 to schedule your consultation today.

6 Comments Posted to "Implant Placement: Over or Under the Muscle?"
Loved it! Got answers I was seeking Thank you
I have had under muscle and am now on my 4th revision operation in 3 years they are under my armpit can see my chest bone when i lie down and sometimes can see the implant when muscle tightens, my surgeon keeps stitching inside saying the picket is too big but it fails everytime within 2 weeks of op, I’m going back next month for the 4th op to stitch sgain , would any one suggest I have him put the inplant over instead I have hand full of skin also like they are not filled properly please someone answer me I’m totally fed up up now and can’t keep going through this
Hi Leanne, we’re sorry to hear about the challenges you’ve been facing with your breast implants. It sounds like you’ve experienced significant difficulties with under-the-muscle placement and the integrity of the implant pocket. It might be beneficial to get a second opinion from a board-certified plastic surgeon who has extensive expertise specifically in breast implant revision. If you live near Eugene or are willing to travel, feel free to schedule a consultation with Dr. Movassaghi so he can hear more about your specific case and discuss your options in person. We understand this has likely been a very long, difficult road for you, and we would love to help you find a solution.
Hi. I wanna ask. lymphoma happen in under or above breast implant? Bcos some say, lymphoma happen when implant is under the muscle. Lymphoma cell can cause cancer is it?
Thank you for your question. It sounds like you are concerned about the condition known as Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL), which is a rare type of non-Hodgkin’s lymphoma that can develop around breast implants. BIA-ALCL is most commonly associated with textured-surface implants rather than placement above or below the muscle, so most plastic surgeons today recommend smooth-surface breast implants regardless of implant placement. If you’re considering implants, discussing your concerns with a board-certified plastic surgeon can provide you with detailed and personalized information to help you make an informed decision.
Hello
I am a nurse practitioner…. I have a patient who had reconstructive surgery after mastectomy. The surgeon basically did a hack job, and she “and her surgical assistant” each did one side… putting one implant under the muscle and one over the muscle. They look AWFUL!!! She told the patient this is normal and they look fine 🫣
On your opinion, is this the gold standard of care??